





















Video
Introduction
If there's one skin concern where a smart routine can deliver visible results relatively quickly, it's pigmentation. I find it genuinely satisfying to treat because when the approach is right, the transformation can be dramatic.
When melanocytes, the cells that produce our skin's pigment, become overactive, they deposit excess melanin in patches, creating uneven skin tone. Our brains are wired to read uniform skin as healthy, which is why these changes bother us even when everything else about our skin is functioning well.
What’s encouraging is that hyperpigmentation responds well to consistent, targeted care. This guide covers everything you need to know to address it effectively - from understanding what's driving your pigmentation to building a routine that works, and knowing when to call in professional help.
What Is Hyperpigmentation?
Hyperpigmentation simply means areas of skin that have become darker than the surrounding tissue. The prefix hyper- simply means "excessive", so we're talking about more pigment production than we want.
Your melanocytes exist to protect you. When your skin perceives a threat - UV exposure being the main one - these cells produce melanin as a defensive shield. They do this via an enzyme called tyrosinase, which acts as the key catalyst in converting amino acids into melanin. That's their job, and it's a good thing. The trouble starts when this protective system becomes overenthusiastic, producing pigment when it doesn't need to, or continuing long after the original trigger has gone.
Understanding this helps explain why pigmentation can feel so stubborn: you're essentially trying to calm down a system that believes it's doing something useful.
The Three Main Types
Not all pigmentation is the same, and knowing which type you're dealing with shapes how you treat it.
Sun Spots (Solar Lentigines)
These are the flat, brown marks that appear on areas with years of sun exposure - common sites are the face, chest, hands, forearms. They're distinct from freckles: larger, more defined, and they don't tend to fade in winter.
Sun spots are essentially your skin's long memory of UV exposure. After decades of cumulative damage, certain melanocytes become permanently switched on, producing pigment in the same locations regardless of current sun exposure. They're extremely common in anyone over 50 with a history of sun exposure.
Post-Inflammatory Hyperpigmentation (PIH)
This is the discolouration left behind after your skin has healed from inflammation, whether that's acne, eczema, a burn, or any other injury. The marks sit exactly where the original problem was.
What's happening here is that inflammation triggers melanin production as part of your skin's healing response. Even after the inflammation resolves, pigment production can continue, leaving a footprint that outlasts the original issue by months or sometimes years.
PIH affects everyone to some degree, but it's more pronounced and persistent in darker skin tones. This is simply because melanocytes in darker skin are more active and responsive - not a flaw, just a characteristic that requires awareness.
One important point: if you're prone to breakouts, resist the urge to pick or scratch. Every time you interfere with a blemish, you're increasing the chance of a longer-lasting pigmented mark in its place.
Melasma
Melasma presents as symmetrical patches of brown or greyish pigmentation, typically across the forehead, cheeks and upper lip. The hallmarks are its map-like appearance and the way it mirrors itself on both sides of the face.
This type is driven largely by hormones. Oestrogen and progesterone sensitise melanocytes, making them hyper-reactive to even minimal UV exposure. This explains why melasma commonly emerges during pregnancy, with oral contraceptive use, or during HRT.
Melasma is significantly more common in people with darker skin tones, particularly those who tan easily (Fitzpatrick skin types III-VI). It affects women far more than men, with only about 10% of cases occurring in males. Genetics play a strong role too; if your family members have melasma, your risk increases substantially.
The frustrating thing about melasma is that the melanocytes involved seem to have a memory. Even after successful treatment, a brief period without sun protection can bring it flooding back. This is why melasma requires ongoing management rather than a one-time fix.
What Drives Pigmentation?
UV Radiation
This is the dominant factor. UV exposure triggers melanin production - that's literally what melanin evolved to do. Sun spots result from cumulative lifetime UV damage. Melasma is triggered and worsened by UV. Post-acne marks darken with sun exposure.
This is why sunscreen isn't just part of a pigmentation strategy; it's the foundation everything else builds on. And yes, that means every single day, year-round: UVA rays penetrate clouds and glass regardless of whether it looks sunny outside.
Visible Light
Recent research shows that visible light from the sun (not screens - that's a myth) can also trigger pigmentation, particularly in darker skin tones. This is why tinted sunscreens containing iron oxide offer additional protection beyond standard UV filters.
Inflammation
Any injury to the skin can trigger pigmentation as part of the healing response. This includes acne, eczema, burns, aggressive skincare, friction.. even mosquito bites. The more intense the inflammation, the more pronounced the resulting pigmentation.
Hormones
Oestrogen and progesterone make melanocytes in susceptible individuals more reactive. Pregnancy, contraceptives, HRT, and even thyroid conditions can all influence pigmentation patterns.
Genetics
Some people simply have melanocytes that are more easily triggered than others. If pigmentation runs in your family, you're more likely to experience it too.
Quick Facts: What's True and What Isn't
SPF is only needed on sunny days – False. UVA penetrates clouds and glass. Daily protection is essential year-round for all types of pigmentation.
Scrubbing helps remove melasma – False. Friction aggravates the hypersensitive melanocytes involved in melasma. Chemical exfoliation (used carefully) is far safer than physical scrubbing.
Once melasma clears, it’s gone for good – False. Melasma is typically chronic and relapsing, requiring ongoing management. Sun spots and PIH, by contrast, can often be fully resolved.
Hydroquinone is dangerous – False, when used correctly. It remains the gold standard treatment for pigmentation. Problems arise from unregulated products at unsafe concentrations. Under medical supervision, it’s both safe and effective.
Screen blue light causes melasma – False. The blue light from devices is negligible compared to sunlight. Visible light from the sun is a different matter – but your phone isn’t something to worry about.
Lasers are the best treatment for melasma – False. Lasers can actually make melasma worse by activating the same pathways that drive the condition. They’re never first-line and require expert assessment.
It’s just cosmetic, not a real concern – False. Pigmentation can significantly impact quality of life and wellbeing. It deserves to be taken seriously.
The Ingredients That Work
We have an excellent toolkit of proven ingredients. Here's what to look for:
Tyrosinase Inhibitors
These block the enzyme needed to produce melanin.
Hydroquinone remains the gold standard, available on prescription. I typically use Hydroquinone 4% strength in my practice. It works relatively quickly and is best used in pulsed cycles under medical supervision.
Azelaic acid is an underrated option – it inhibits pigment production while also calming inflammation. Available over the counter at 10% or prescription strength at 15-20%. Safe in pregnancy, which makes it particularly valuable, when other concerns like acne or rosacea are also present.
Vitamin C modestly inhibits tyrosinase while providing antioxidant protection. L-ascorbic acid at 10-15% is the most studied form, though it can be unstable and irritating for some. More stable vitamin C esters include THD ascorbate (oil-soluble, excellent for dry skin), ascorbyl glucoside (gentle, good for sensitive skin), and magnesium ascorbyl phosphate (water-soluble and well-tolerated). Best used in the morning alongside SPF - I think of it as being a key anchor in pigmentation prevention, rather than a complete solution in and of itself.
Hexylresorcinol is a potent tyrosinase inhibitor that also has antioxidant properties. It’s often found in combination products and is well-tolerated, even by sensitive skin.
Niacinamide works differently – it blocks the transfer of melanin to skin cells rather than blocking production. Extremely well tolerated. The sweet spot is 5-10%.
Arbutin is a gentle tyrosinase inhibitor derived from bearberry. Slower to show results but useful for sensitive skin.
Kojic acid and kojic dipalmitate are derived from fungi and inhibit tyrosinase effectively. Kojic dipalmitate is the more stable, less irritating form of the two, making it a more suitable choice for sensitive skin and melanated skin.
Cell Turnover Accelerators
These help shed pigmented cells faster.
Retinoids speed up epidermal renewal, helping pigmented cells turn over more quickly. They also suppress melanin production directly. Use at night, always with daytime SPF.
Bakuchiol offers a plant-derived alternative for those who can’t tolerate retinoids or need to avoid them (such as during pregnancy). It has potent longevity benefits as an antioxidant and anti-inflammatory agent, alongside its retinoid-like effects on cell turnover - and it also tends to reduce tyrosinase activity, making it a genuinely useful addition to the pigmentation toolkit.
Alpha hydroxy acids (AHAs) like glycolic and lactic acid dissolve bonds between cells, encouraging shedding of pigmented surface cells. Lactic acid is the gentler option with added hydrating benefits. Use with caution - over-exfoliation causes inflammation, which triggers more pigmentation.
The Non-Negotiable
Broad-spectrum SPF 50 - without this, everything else is wading through treacle. For melasma-prone skin or darker skin tones, consider tinted formulas with 1-3 % iron oxide for visible light protection too.
An Inside-Out Approach
Skincare supplements are often a grey area but there are promising clinical studies that some ingredients can help improve hyperpigmentation.
Polypodium leucotomos is a very interesting fern extract from South America with antioxidant and photo-protective properties that help shield against the harmful effects of the sun. Whilst it’s best taken alongside a structured skincare routine, the supplement showed promising results in a small trial to improve melasma control in those who took it at a dose of 240mg twice a day.
Building Your Routine
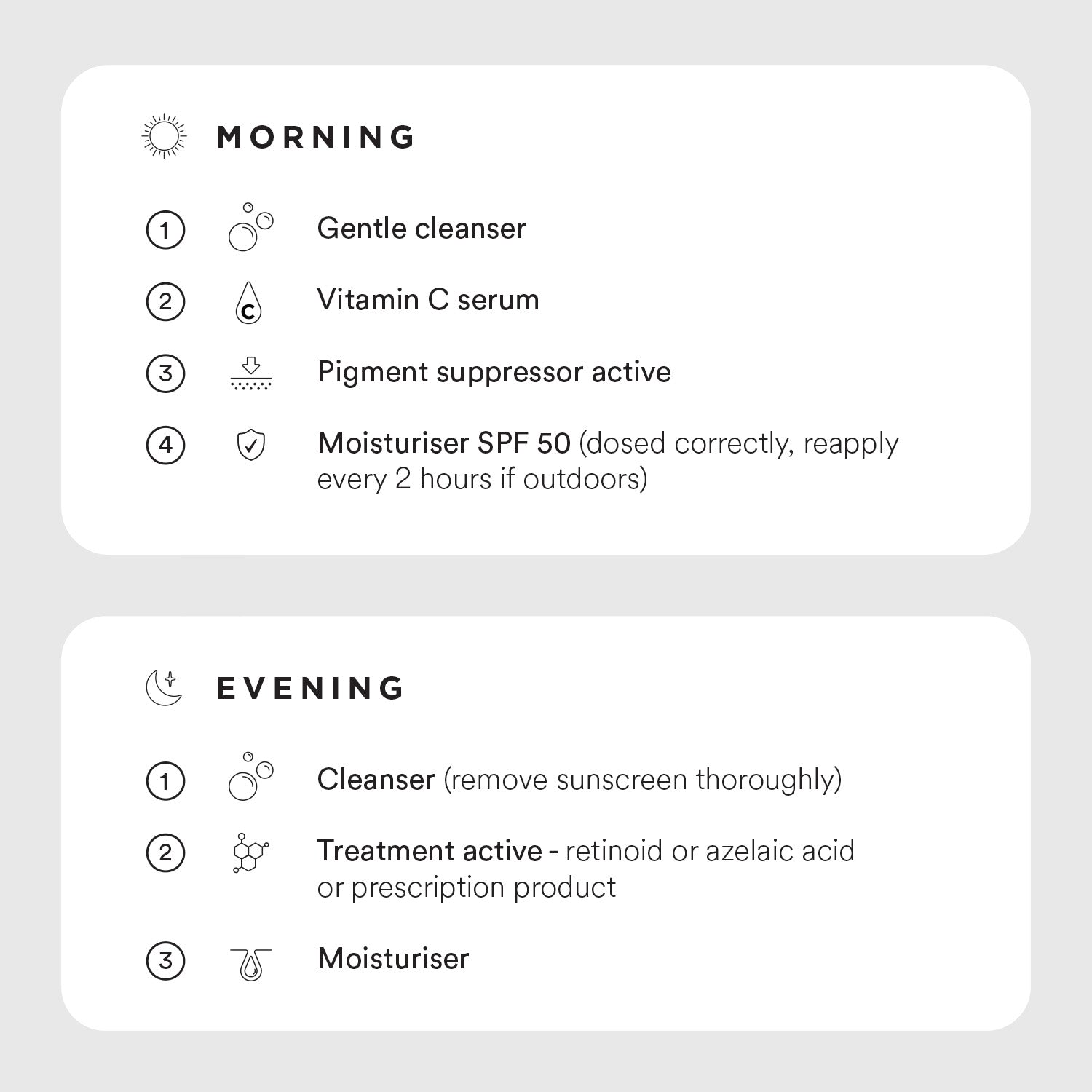
Key Principles
Introduce one active at a time. Give your skin 2-4 weeks to adjust before adding anything new. You want to avoid irritation and the risk of PIH.
Patience is essential. Expect initial improvements around 4-8 weeks, meaningful change at 3-6 months. Melasma requires ongoing management indefinitely.
Protect relentlessly. Sun exposure undoes progress quickly. SPF every single day.
Avoid irritation. Redness, tightness, flaking - these are signs you've overdone it. Irritation causes inflammation, which causes more pigmentation. Scale back if needed.
Don't make matters worse. When you have a skin concern, a quick-fix can be tempting but faster often means increased risk. I’ve seen too many patients regret laser treatment for melasma or microdermabrasion for acne. This also applies to breakouts - if you pick or scratch your pimples you’re going to create a lot more pigmentation than if you just left it be!
Considerations for Darker Skin Tones
Hyperpigmentation affects people with darker skin more frequently and more intensely. PIH lasts longer. Melasma is more common. This reflects the fact that melanocytes in darker skin are simply more active - not a problem, just a characteristic that requires adapted care.
Start gently. Darker skin is more reactive to irritation, and irritation triggers PIH. Begin with lower concentrations and increase gradually.
Prioritise anti-inflammatory ingredients. Azelaic acid and niacinamide are particularly valuable because they calm inflammation while addressing pigmentation.
Be cautious with procedures. Chemical peels and lasers carry higher risk of post-procedure hyperpigmentation in darker skin. If considering these, ensure your practitioner has specific experience with skin of colour.
Use visible light protection. Tinted sunscreens with iron oxide are more effective than UV-only sunscreens for preventing melasma relapse in darker skin tones.
Expect treatment to take longer. Results are often more gradual. Consistency matters more than intensity.
When to See a Dermatologist
A consistent home routine works well for many people, but professional help is warranted when you've seen no improvement after 3-6 months of consistent treatment or you're dealing with melasma (prescription options are often more effective).
It’s also recommended if your pigmentation appeared suddenly or is changing in appearance. Any individual pigmented lesion which looks irregular, has uneven colour, or is evolving should be reviewed to rule out a type of skin cancer called melanoma.
Finally, if the condition is significantly affecting your wellbeing, chatting to an expert can offer enormous relief.
A dermatologist can prescribe stronger treatments, assess whether procedures might help your specific situation, and ensure you're not missing anything important.

Frequently Asked Questions
How long does hyperpigmentation take to fade? This varies by type and depth. Superficial PIH from a recent spot might fade in 1-6 months with good treatment and sun protection. Deeper pigmentation can take years. Melasma requires ongoing management rather than expecting complete resolution.
Can it be permanently cured? Sun spots and PIH can often be fully resolved. Melasma is typically chronic - it can be controlled but tends to recur without ongoing care.
Why does my pigmentation get worse when I'm treating it? Usually this means either inadequate sun protection or irritation from treatment. Scale back your actives, focus on barrier repair, and be rigorous with SPF. Pigmentation that's being irritated will darken before it improves.
Can I use vitamin C and retinoids together? Yes, though if you're new to actives, introduce them separately. Many people use vitamin C in the morning and a retinoid at night without problems. If that's too much, alternate nights.
Is pigmentation more common in darker skin? PIH and melasma are more common and more pronounced in darker skin tones. The same treatments work, but the approach needs to be gentler to avoid triggering further pigmentation through irritation.
The Bottom Line
Pigmentation responds well to the right approach. The essentials are:
- Daily SPF - the foundation of everything
- Proven actives - retinoids, azelaic acid, niacinamide, vitamin C
- Patience and consistency - results come with time
- Avoiding irritation - inflammation makes pigmentation worse
- Realistic expectations - especially with melasma, this is about management, not cure
Remember: your skin can improve dramatically with consistent, targeted care.
References
1.McKesey J, Tovar-Garza A, Pandya AG. Melasma Treatment: An Evidence-Based Review. Am J Clin Dermatol.2020;21(2):173-225. PMID: 31802394
2.Sarkar R, et al. Topical and Systemic Therapies in Melasma: A Systematic Review. Indian Dermatol Online J.2023;14(6):769-781. PMID: 38099013
3.Tan MG, et al. Topical treatment for postinflammatory hyperpigmentation: a systematic review. J Dermatolog Treat. 2022;33(5):2518-2526. PMID: 34525885
4.Silpa-Archa N, et al. Postinflammatory hyperpigmentation: A comprehensive overview. J Am Acad Dermatol.2017;77(4):591-605. PMID: 28917451
5.Castanedo-Cazares JP, et al. Near-visible light and UV photoprotection in the treatment of melasma: a double-blind randomized trial. Photodermatol Photoimmunol Photomed. 2014;30(1):35-42. PMID: 24313385
6.Zhou C, et al. Guide to tinted sunscreens in skin of color. Int J Dermatol. 2024;63(3):272-276. PMID: 38073075
7.Lyons AB, et al. Photoprotection beyond ultraviolet radiation: A review of tinted sunscreens. J Am Acad Dermatol.2021;84(5):1393-1397. PMID: 32335182
8.Callender VD, et al. Postinflammatory hyperpigmentation: etiologic and therapeutic considerations. Am J Clin Dermatol. 2011;12(2):87-99. PMID: 21348540
9.Davis EC, Callender VD. Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 2010;3(7):20-31. PMID: 20725554
10.Kaufman BP, et al. Postinflammatory hyperpigmentation: epidemiology, clinical presentation, pathogenesis and treatment. Am J Clin Dermatol. 2018;19(4):489-503. PMID: 29222629
11. Ahmed AM, Lopez I, Perese F, Vasquez R, Hynan LS, Chong B, Pandya AG. A randomized, double-blinded, placebo-controlled trial of oral Polypodium leucotomos extract as an adjunct to sunscreen in the treatment of melasma. JAMA Dermatology. 2013;149(8):981–983. doi:10.1001/jamadermatol.2013.4294. PMID: 23740292
{kind=link}
Related Articles

Melasma Treatment : A London Dermatologist's Guide to Bright, Clear Skin
Summer in London can be glorious. But for many of my patients, this is also the time of year when melasma makes its unwelcome return. It’s a condition that, once triggered, often becomes a chronic ...

7 Things This Dermatologist Wants You To AVOID If You Have PIGMENTATION!
Have you ever met anyone who is happy with their pigmentation? It’s certainly become the aspect of ageing that my patients are keenest to address. And I think that’s because we’re hardwired to lik...

A Dermatologist's Guide To Treating Melasma - Update!!!
I see more patients for hyperpigmentation than ever before - women (and men) are really starting to grasp that addressing uneven skin tone is a powerful beauty fix. Lines and wrinkles matter much ...